Project
Ultra-Low Dose CT for Novel Screening Applications
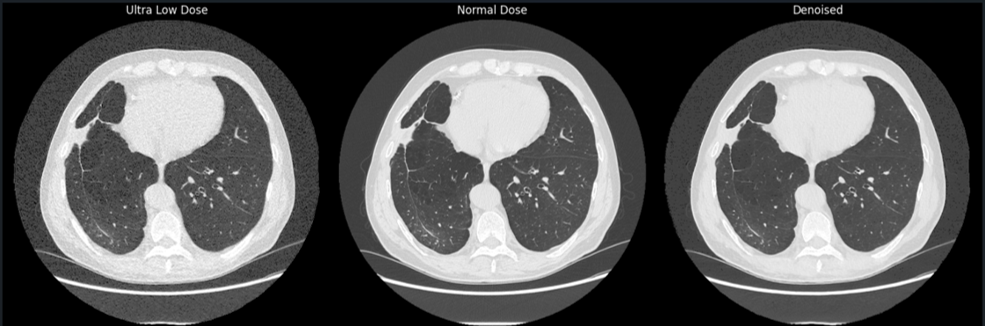
Radiologic screening of the future: the case for computationally enhanced ultra-low dose CT — bringing any existing CT scanner down to the radiation level of a plain X-ray to unlock a new generation of population screening.
The ideal modality for imaging based screening does not exist...
“Screening is the process of using tests on a large scale to identify the presence of disease in apparently healthy people”[1]. At population scale, the implemented screening technique must be accessible, low-cost, and safe. Yet in half a century the US has fielded only a handful of large-scale, reimbursed imaging-based screening programs — mammography (1976), osteoporosis DEXA (1998), and low-dose CT for lung cancer (2015).
Every existing modality trades strengths against weaknesses. For example, CT offers rich 3D information at low cost and high availability, but its ionizing radiation has kept it off the screening table for most applications.
| Modality | Cost | 2D / 3D | Repeatability | Ionizing radiation | Availability |
|---|---|---|---|---|---|
| X-ray | Low | 2D | Medium | Very low | High |
| Ultrasound | Low | 2D (mainly) | Low | None | High |
| CT | Low | 3D | High | High | High |
| MRI | High | 3D | High | None | Low |
| PET/CT-MR | High | 3D | High | High | Low |
Our approach: AI-enhanced ultra-low dose CT
The vision is to bring any existing, low-cost CT scanner down to the radiation level of a 2D X-ray — turning radiation exposure into a non-issue — and thereby enable entirely new screening applications.
The motivation is concrete: CT screening for lung cancer was proven to reduce mortality by ~20%[2], and annual low-dose lung screening CT is reimbursed for at-risk populations in the US, amounting to some 17 million scans per year[3]. But “low dose” is still ~1 to 1.5 mSv — the equivalent of about 10-15 chest X-rays. Following the ALARA principle (As Low As Reasonably Achievable), the goal is to close that gap.
Building a unique dataset
Supervised denoising needs paired ultra-low-dose and normal-dose scans of the same patient — a dataset that simply did not exist. There are two ways to obtain one:
- Retrospective — add synthetic noise to existing normal-dose scans. One scan per patient, aligned by design, no consent required — the noise is simulated.
- Prospective — acquire real pairs of ULD and normal-dose scans. Two scans per patient, requiring informed consent and non-rigid registration — the noise is real.
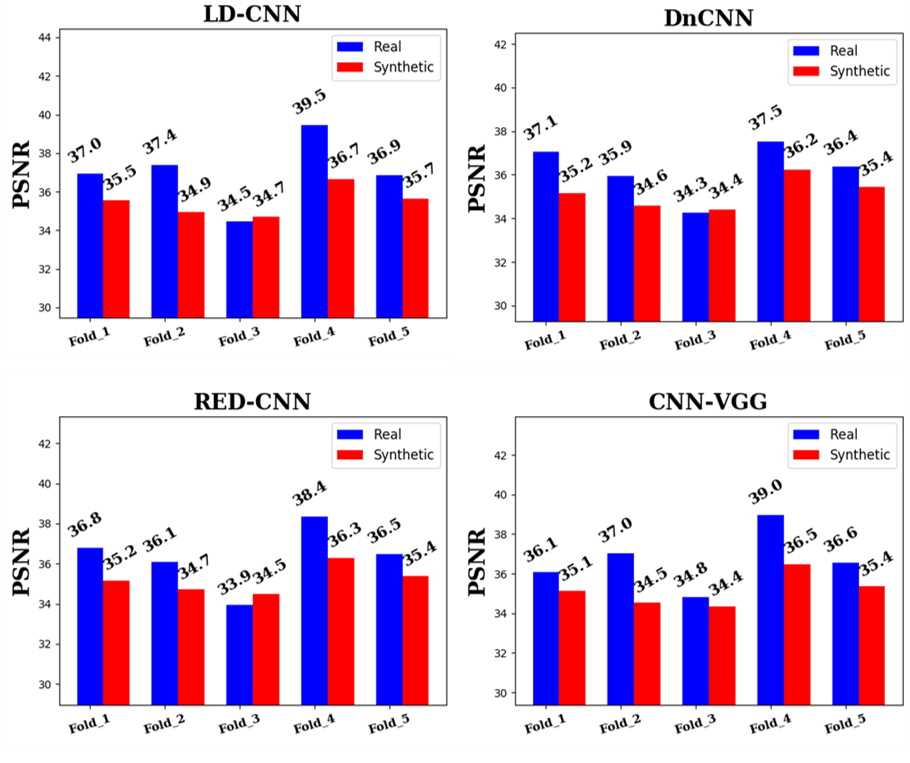
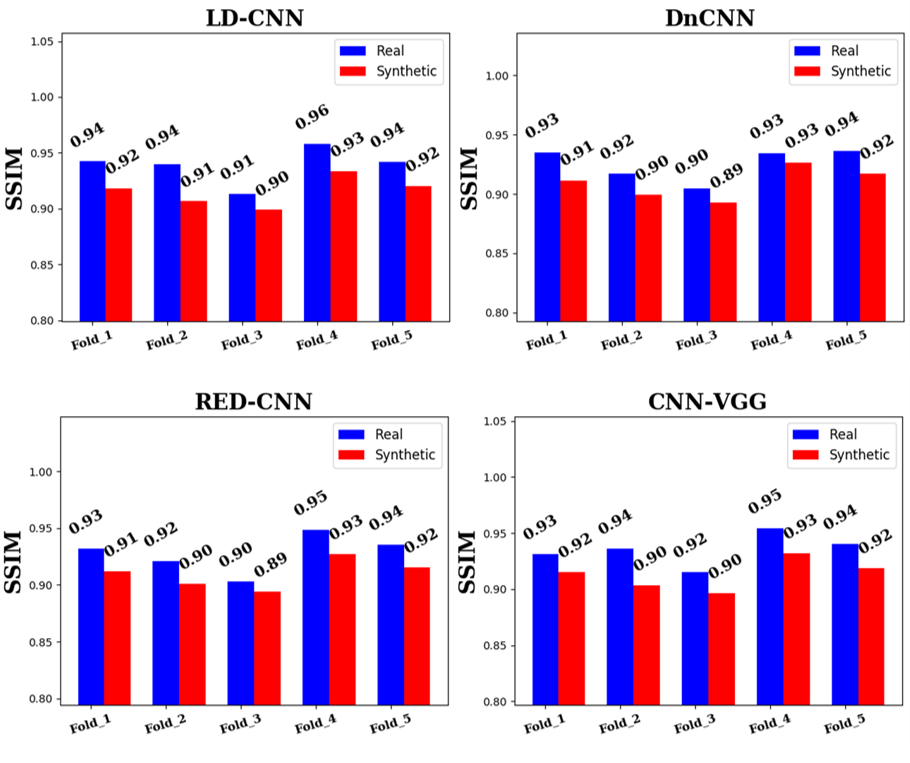
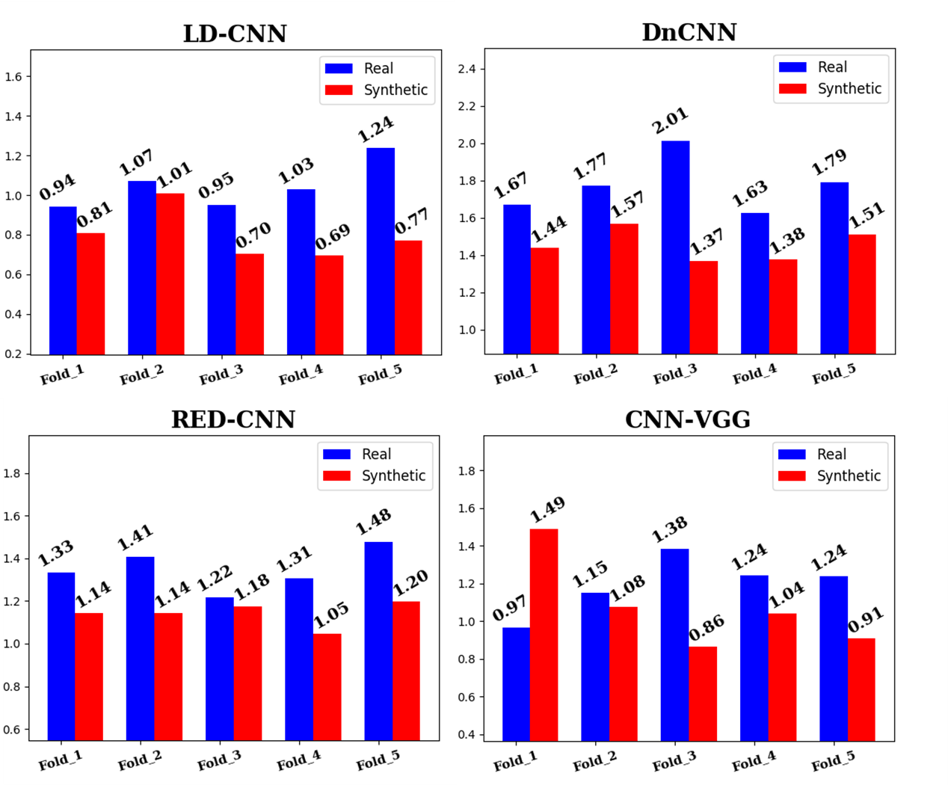
Real noise matters: we have shown[4] that models trained on genuinely acquired ULD noise achieve significantly higher Peak-SNR, higher structural similarity (SSIM), and higher S3 sharpness (all statistically significant) than those trained on synthetic noise.
Because a patient never holds exactly the same full inspiration twice, each ULD scan is brought into alignment with its normal-dose ground truth through affine + deformable registration (Elastix).

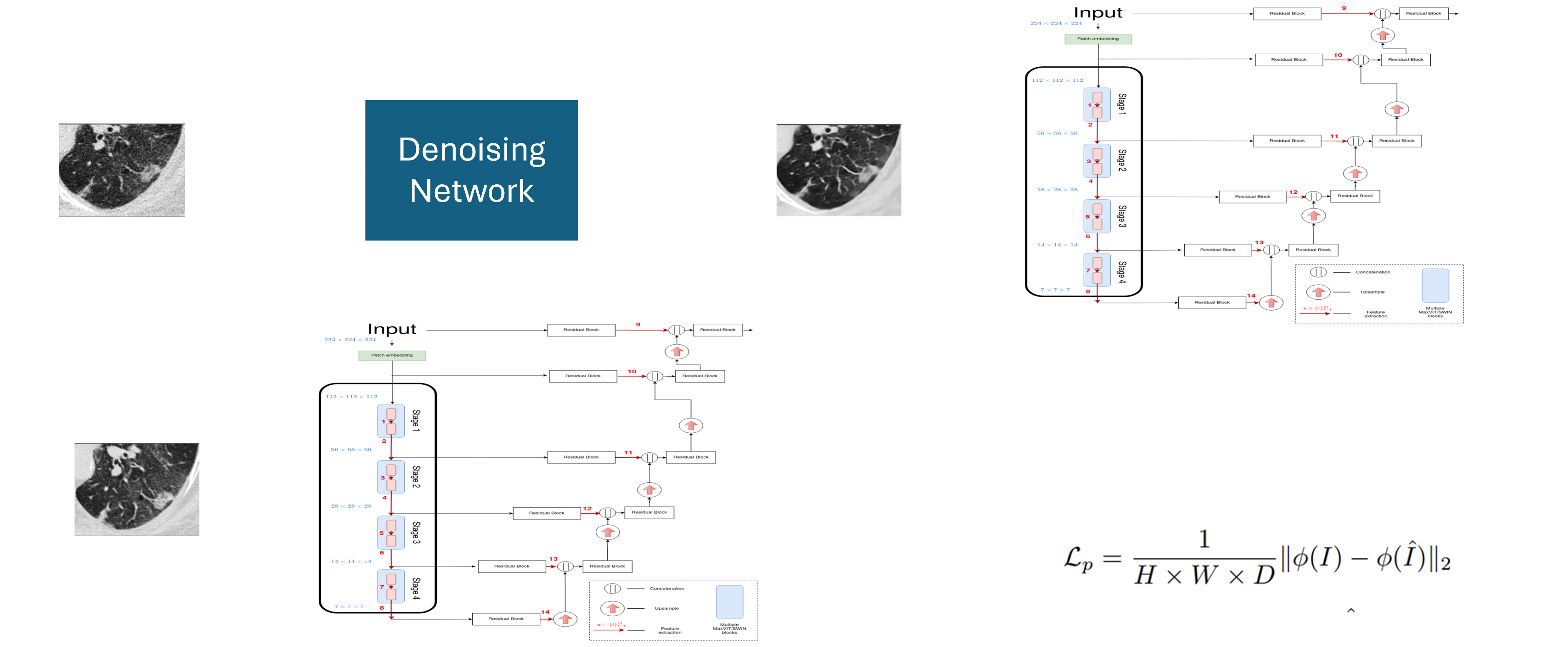
The denoising engine: the trick is in the loss!
The denoising network is trained with a perceptual loss — comparing denoised and ground-truth patches inside a learned embedding space rather than pixel-by-pixel. The lab's approach evolved from a convolutional perceptual loss (ISBI 2019[5]) to the Perceptual Transformer Loss (PeTeL) built on a 3-D MaxViT backbone combining block and grid self-attention, which achieves superior quantitative and qualitative denoising (ISBI 2024[6]).
One scan, four indications
A single AI-denoised ultra-low dose acquisition currently supports four different clinical indications.
Bibliography
- Bonita, R., Beaglehole, R. and Kjellström, T., 2006. Basic epidemiology. World Health Organization. ↩
- The National Lung Screening Trial Research Team, 2011. Reduced lung-cancer mortality with low-dose computed tomographic screening. New England Journal of Medicine, 365(5), pp.395–409. doi:10.1056/NEJMoa1102873. ↩
- US Preventive Services Task Force, 2021. Screening for lung cancer: US Preventive Services Task Force recommendation statement. JAMA, 325(10), pp.962–970. doi:10.1001/jama.2021.1117. ↩
- Green, M., Marom, E.M., Konen, E., Kiryati, N. and Mayer, A., 2018. Learning real noise for ultra-low dose lung CT denoising. In International Workshop on Patch-based Techniques in Medical Imaging (pp. 3–11). Cham: Springer International Publishing. ↩
- Green, M., Marom, E.M., Konen, E., Kiryati, N. and Mayer, A., 2019. Feature aggregation in perceptual loss for ultra low-dose (ULD) CT denoising. In 2019 IEEE 16th International Symposium on Biomedical Imaging (ISBI) (pp. 1635–1638). IEEE. ↩
- Green, M., Marom, E.M. and Mayer, A., 2024. Perceptual transformer loss for the neural denoising of ultra-low dose CT. In 2024 IEEE International Symposium on Biomedical Imaging (ISBI) (pp. 1–5). IEEE. doi:10.1109/ISBI56570.2024.10635771. ↩
- Gorenstein, L., et al., 2023. A novel artificial intelligence based denoising method for ultra-low dose CT used for lung cancer screening. Academic Radiology. ScienceDirect. ↩
- Kerpel, A., Marom, E.M., Green, M., Eifer, M., Konen, E., Mayer, A. and Betancourt Cuellar, S.L., 2021. Ultra-low dose chest CT with denoising for lung nodule detection. Israel Medical Association Journal, 23(9), pp.550–555. link. ↩
- Klug, M., Shemesh, J., Green, M., Mayer, A., Kerpel, A., Konen, E. and Marom, E.M., 2022. A deep-learning method for the denoising of ultra-low dose chest CT in coronary artery calcium score evaluation. Clinical Radiology, 77(7), pp.e509–e517. doi:10.1016/j.crad.2022.03.005. ↩
- Kirshenboim, Z., Marom, E.M., Mayer, A., Green, M., Klug, M. and Tau, N., 2022. Liver attenuation assessment in reduced radiation chest computed tomography. Journal of Computer Assisted Tomography, 46(5), pp.682–687. doi:10.1097/RCT.0000000000001340. ↩
- Klug, M., Sobeh, T., Green, M., Mayer, A., Kirshenboim, Z., Konen, E. and Marom, E.M., 2025. Denoised ultra-low-dose chest CT to assess pneumonia in individuals who are immunocompromised. Radiology: Cardiothoracic Imaging, 7(2), e240189. doi:10.1148/ryct.240189. ↩