Project
Automatic Deep Inferior Epigastric Perforator Mapping for Breast Flap Surgery
An end-to-end deep learning pipeline that reads an abdominal CTA scan, labels the anatomy of the abdominal wall, and pinpoints the perforator vessels a reconstructive surgeon must find — replacing hours of manual annotation with under ten minutes of computation.
The DIEP flap, and where it gets stuck
After a mastectomy, breast reconstruction can be done with an implant or with the patient's own tissue. The autologous option that has become the gold standard is the DIEP flap — Deep Inferior Epigastric Perforator flap — in which skin and fat are taken from the lower abdomen and transplanted to the chest to rebuild the breast. It gives a natural result that ages with the patient, and, unlike older techniques, it spares the rectus abdominis muscle entirely, so abdominal strength is preserved.
Sparing the muscle is exactly what makes the operation hard. The transplanted tissue must stay alive, which means it must carry its own blood supply with it. That supply arrives through perforators: small branches of the deep inferior epigastric artery that pierce through the rectus abdominis muscle and its fascia and fan out into the overlying fat. The surgeon has to trace one of these vessels through the muscle without cutting the muscle — a dissection that can only be planned if the vessel's course and its perforation point are known in advance.
Current practice: hours of manual reading
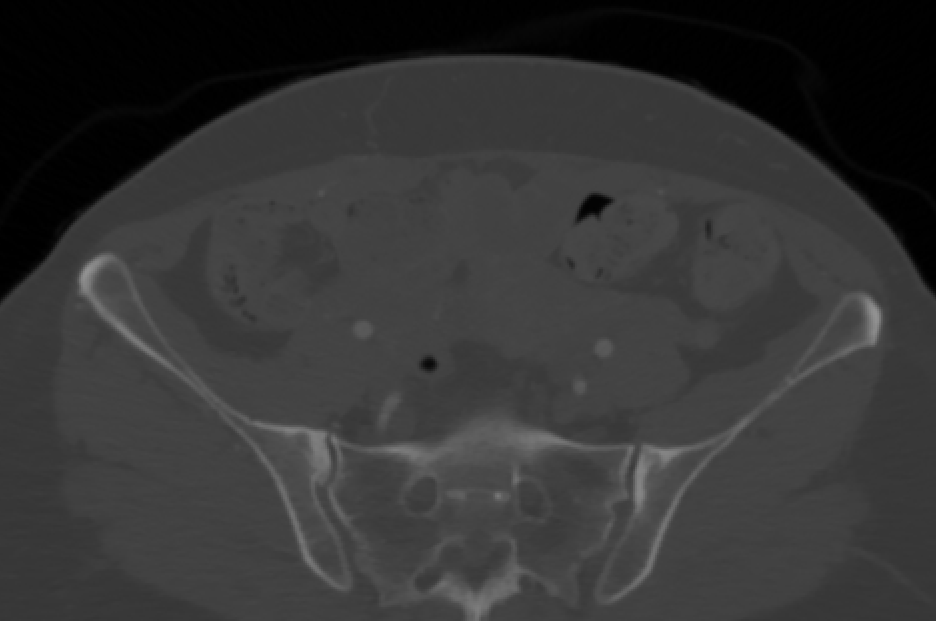
Planning starts with a contrast-enhanced CT angiography (CTA) scan of the abdomen. Somewhere in those hundreds of slices are the perforators — each one a bright dot barely a couple of millimetres across, visible for only a handful of slices as it crosses the fascia.
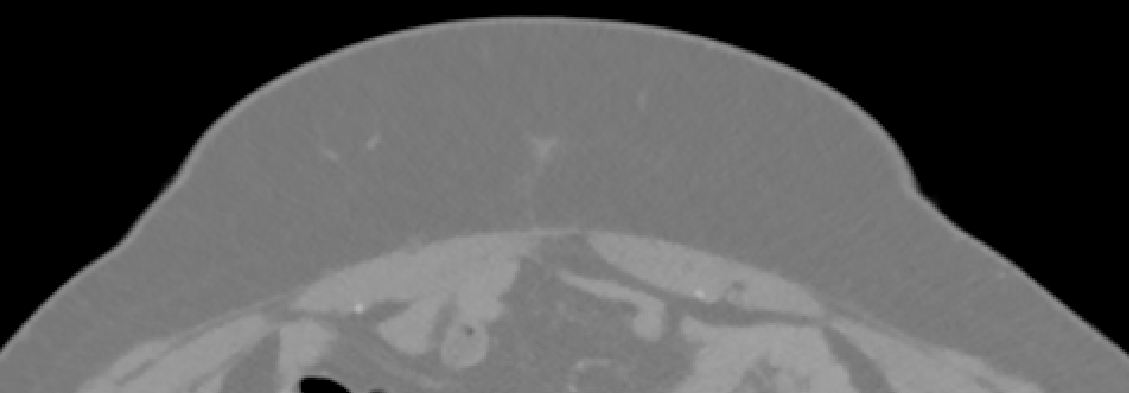
A radiologist or surgeon scrolls the volume, marks candidate vessels slice by slice, measures each one's calibre and its distance from the umbilicus, and reconstructs its path through the muscle. The result is a hand-drawn map of which perforator to use and where to cut. It is accurate, but it takes hours per case, it depends heavily on the reader's experience, and it does not scale — which is why many centres do it only partially, or not at all.
Our goal: an automatic pipeline from scan to plan
We set out to automate the whole path — raw CTA in, surgical map out — with no manual step in between. The pipeline chains five stages, and the intermediate anatomical segmentation is what makes the last one tractable: rather than hunting for bright dots across the entire abdomen, the vessel search is confined to the tissue where perforators actually live.
Data
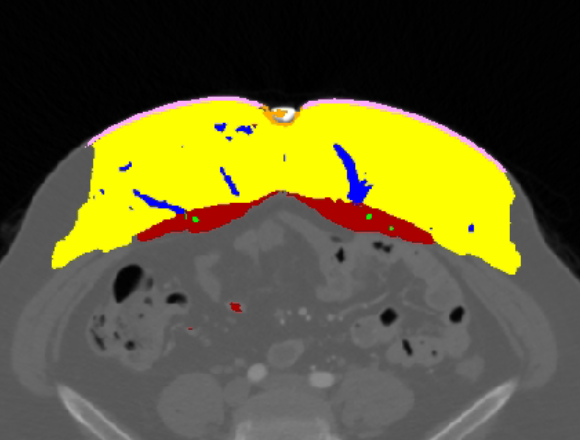
34 abdominal CTA scans were collected retrospectively at Sheba Medical Center from patients who underwent DIEP flap reconstruction, acquired on Philips iCT 256 and Ingenuity scanners. Each scan was annotated by hand into six anatomical classes, plus the ground-truth perforation points.
- Subcutaneous fat
- Rectus abdominis muscle
- DIEA & INTRA
- SIEA
- Skin
- Umbilicus
The vessel classes are the ones that carry the surgical decision. The DIEA (deep inferior epigastric artery) and its intramuscular branches are the source of the perforators the DIEP flap is built on; the SIEA (superficial inferior epigastric artery) is the alternative supply a surgeon may fall back on. The umbilicus matters because it is the anatomical landmark against which perforator positions are reported in the operating room.
Volumes were resampled to a uniform grid — 2 mm slice spacing at 0.69 × 0.69 mm in plane — so that the network sees consistent geometry across scanners and acquisitions. The 34 cases were split into 25 for five-fold cross-validation (20 training and 5 validation per fold) and 9 held out as an independent test set.
Method
Two SwinUNETRs, in sequence
The abdominal wall occupies a small fraction of a CTA volume, and the structures of interest are thin. Feeding the whole scan to a segmentation network at full resolution wastes most of its capacity on irrelevant anatomy. So we use SwinUNETR twice: once to find where to look, and once to label what is there.
The first network extracts the region of interest — the anterior abdominal wall between skin and peritoneum. The second network takes that cropped region and produces the full six-class segmentation. Both are initialised from Swin transformer weights pre-trained on the BTCV abdominal dataset, then fine-tuned for 100 epochs with a Dice loss and the Adam optimiser, at batch size 1. The implementation uses PyTorch and MONAI, and trains on a single NVIDIA RTX A5000 (24 GB).
From voxels to perforation points
A segmentation mask of the vessel tree is not yet an answer. What the surgeon asks for is a short list of points — the coordinates at which each usable perforator pierces the fascia. To get there, we take the predicted vessel voxels that sit at the muscle boundary and group them with DBSCAN, a density-based clustering algorithm that requires no guess at how many perforators exist and discards isolated voxels as noise. 3D connected component analysis then resolves each cluster into a distinct perforator and yields its perforation point.
This is where the earlier anatomical segmentation pays off: because the muscle and fat boundaries are already known, a candidate is only considered where a perforator is anatomically possible, and the vast majority of spurious bright voxels elsewhere in the scan never enter the clustering at all.
Results
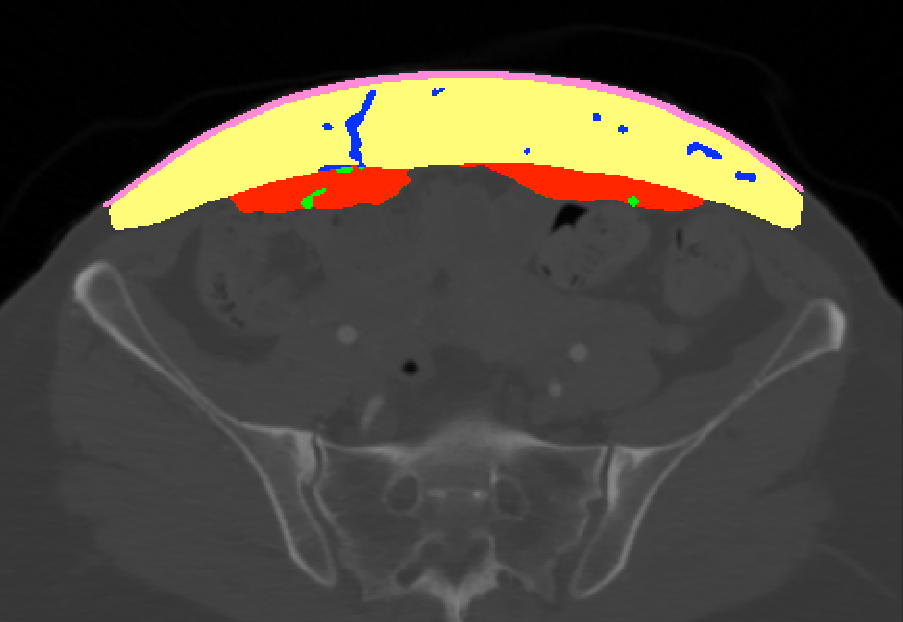
Anatomical segmentation
The fully automatic pipeline — with the region of interest found by the first network rather than given by a human — reaches an overall Dice score of 0.84 across the six classes.
| Anatomical class | Dice ↑ |
|---|---|
| Skin | 0.92 |
| Subcutaneous fat | 0.88 |
| Rectus abdominis muscle | 0.87 |
| SIEA | 0.85 |
| DIEA & INTRA | 0.78 |
| Umbilicus | 0.75 |
| Overall | 0.84 |
The ordering is anatomically unsurprising. Skin and fat are large, high-contrast and consistent, and score highest. The vessels and the umbilicus are small structures whose Dice is dominated by a thin boundary — a one-voxel disagreement costs a large fraction of the score on a two-voxel-wide artery, which is why 0.78 on the DIEA is a stronger result than it looks next to 0.92 on skin.
Perforator detection
Segmentation quality is a proxy; what matters clinically is whether the right perforation points come out. Across the evaluated cases there were 112 ground-truth perforation points. Detection is scored against a distance tolerance: a predicted point counts as a hit if it lands within a given radius of a true one. At the 5 mm tolerance selected as clinically meaningful by our surgical collaborators, the pipeline finds 76 of the 112 points (67.9%), with a mean localisation error of 1.71 mm on those it finds. Over the full range of operating points, the precision–recall curve gives an average precision of 0.71.
Those two numbers describe different things, and both matter. The 67.9% is a recall figure — a third of the annotated perforators are still missed. The 1.71 mm is a precision-of-placement figure, and it is comfortably inside the tolerance the surgeon works to: when the pipeline does find a perforator, it puts it in very nearly the right place.
Discussion & outlook
The result we care about most is not any single score — it is that the path from a raw CTA to a labelled perforator map runs end to end without a human, in under ten minutes, against a manual workflow measured in hours. That changes what is practical: planning can be done for every case rather than for the ones there is time for, and the surgeon's reading time shifts from finding vessels to choosing between them.
The honest limitation is recall. At the clinical tolerance the pipeline still misses roughly a third of the annotated perforation points, so it is a planning aid to be reviewed, not a replacement for the surgeon's read. The cohort is also small — 34 scans from a single centre and two scanner models — and the vessel classes are exactly the ones a small cohort teaches least well.
The clearest routes forward follow from that: more cases and more centres; a detection stage trained directly against the perforation points rather than inheriting them from a segmentation mask; and taking the map the last step into the operating room, as intra-operative navigation rather than a document read beforehand.
This work was presented at the 2026 IEEE International Symposium on Biomedical Imaging (ISBI), London, UK, April 8–11, 2026.
References
- S. Ashkenazi, N. Kiryati, D. Freidin, R. Zarik, A. Tessone, S. Tejman-Yarden, and A. Mayer, "Abdominal Segmentation and Blood Vessel Detection in CTA Scans for DIEP Reconstruction Procedures," IEEE International Symposium on Biomedical Imaging (ISBI), London, UK, 2026.
- A. Hatamizadeh, V. Nath, Y. Tang, D. Yang, H. R. Roth, and D. Xu, "Swin UNETR: Swin Transformers for Semantic Segmentation of Brain Tumors in MRI Images," MICCAI BrainLes Workshop, 2021.
- Y. Tang, D. Yang, W. Li, H. R. Roth, B. Landman, D. Xu, V. Nath, and A. Hatamizadeh, "Self-Supervised Pre-Training of Swin Transformers for 3D Medical Image Analysis," IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), 2022.
- M. Ester, H.-P. Kriegel, J. Sander, and X. Xu, "A Density-Based Algorithm for Discovering Clusters in Large Spatial Databases with Noise," International Conference on Knowledge Discovery and Data Mining (KDD), 1996.
- M. J. Cardoso et al., "MONAI: An open-source framework for deep learning in healthcare," arXiv:2211.02701, 2022.